This article addresses the question “Why should Veterans’ advocates care that Agent Orange exposed Veterans are over twice as likely as unexposed Veterans to be diagnosed with the generally asymptomatic disease MGUS?” Recent research by scientists at the NIH, CDC, and others that showed that MGUS is significantly more prevalent in Agent Orange exposed Veterans is described in a previous post. Why is this a big deal?
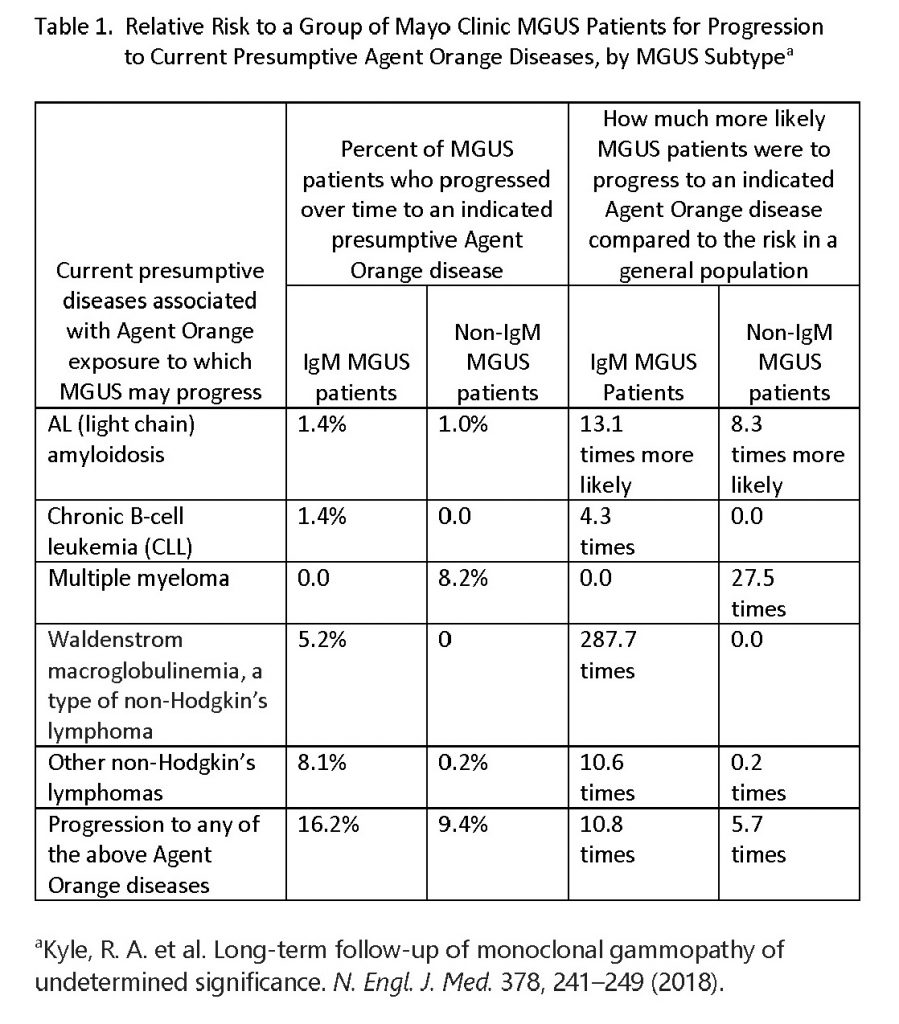
Findings of recent research by Mayo Clinic scientists that answer our question are presented in Table 1 below. This research quantified the percentage of Mayo Clinic patients with either of the two major biologic subtypes of MGUS (IgM MGUS and non-IgM MGUS) who progressed to each of five diseases that are on the current presumptive Agent Orange list over a 34 year period.
Significantly, lifelong monitoring of patients with MGUS showed that almost one in six (16.2 percent) of IgM MGUS patients and more than one in eleven (9.4 percent) of non-IgM MGUS patients progressed to an Agent Orange disease during the study period. IgM MGUS patients were 13.1 times more likely and non-IgM patients were 8.3 times more likely to be subsequently diagnosed with the deadly Agent Orange disease AL (light chain) amyloidosis compared to a general population served by the Mayo Clinic.
Moreover, non-IgM MGUS patients were 27.5 times more likely to be diagnosed with the often painful Agent Orange disease multiple myeloma. While multiple myeloma remains incurable, in recent years new therapeutic agents have been approved for multiple myeloma which has led to a significant improvement in survival, particularly if the disease is diagnosed early.
IgM MGUS patients were 287.7 times more likely to be diagnosed with the incurable Agent Orange disease Waldenstrom macroglobulinemia and 10.6 times more likely to be diagnosed with other non-Hodgkin’s lymphomas. As with multiple myeloma, it is an exciting time for Waldenstrom macroglobulinemia therapy development with novel and promising treatment options on the horizon.
Research has shown that the health outcomes of MGUS patients are likely to be better when MGUS patients are aware they have MGUS and when they are are monitored for progression and complications by their healthcare provider. It is for this reason that the Chief of Myeloma Service at Memorial Sloan Kettering Cancer Center in New York, Dr. Ola Landgren, (and the lead author of the research first mentioned above) has recommended that Agent Orange exposed Veterans be screened for MGUS.
In fact, because of the significance of MGUS, a research team has recently invited over 140,000 of Iceland’s citizens to be screened to see if they have MGUS to confirm the hypothesis that nation-wide screening for MGUS is beneficial. Those diagnosed with MGUS are being invited to participate in a large randomized clinical trial to determine the optimum way to monitor (follow-up) MGUS patients for progression and complications. One arm of the randomized clinical trial is assessing a more intensive lifetime MGUS monitoring regime that includes regular blood and urine tests for AL amyloidosis, which is often not diagnosed until it is too late. This regime reflects the reality documented by an international expert in diagnosis and treatment of amyloidosis at the Mayo Clinic, Dr. Morie Gertz, that “At Mayo Clinic, 9% of all patients seen with a monoclonal gammopathy are ultimately proven to have light chain amyloidosis. Even adjusting for referral bias, 3–4% of all patients with monoclonal proteins seen have light chain amyloid. Furthermore, if a provider does not see one patient with AL amyloidosis for every five patients with multiple myeloma, it is likely the diagnosis is being overlooked.”
So, the answer to the above question is as follows: Veterans’ advocates should care that Agent Orange exposed Veterans are much more likely to have the pre-malignant disease MGUS because life-long monitoring of MGUS patients and earlier interventions using recently-discovered therapies are likely to improve Veteran health outcomes. As was noted above, progression to the current Agent Orange diseases listed in Table 1 are much more likely to occur among MGUS patients than in the general population. In accordance with US law, Veterans should be offered no-cost VA healthcare for monitoring of MGUS for progression and complications, and treatment of MGUS to prevent progression to current Agent Orange diseases or complications, if medically appropriate.
If you do care, take up this advice of the famous American cultural anthropologist, Margaret Mead: “Never doubt that a small group of thoughtful, committed, citizens can change the world. Indeed, it is the only thing that ever has.” Then join the Vietnam Veterans of America in asking your members of Congress to support bills that would add MGUS to the Agent Orange presumptive list.